

Why Your Thyroid Results Come Back "Normal" — But You Still Feel Terrible


You’ve ticked all the boxes. You went to your GP or Primary Care Physician and asked about your thyroid, had the blood test, and waited. The results came back and the doctor said everything looks fine. Normal. Nothing to worry about.
But you’re exhausted. You’re gaining weight despite eating well. Your hair is coming out in the shower. You’re cold when everyone else is comfortable. Your brain feels like it’s running through fog. And you have this constant, low-level feeling that something just isn’t right with your body.
If that sounds familiar, you’re not imagining it. And you’re far from alone.
The problem isn’t necessarily that your thyroid is broken. The problem is that the standard UK NHS and US thyroid test only tells part of the story — and for a significant number of people, the part it’s missing is exactly where things are going wrong.
What the standard test actually measures
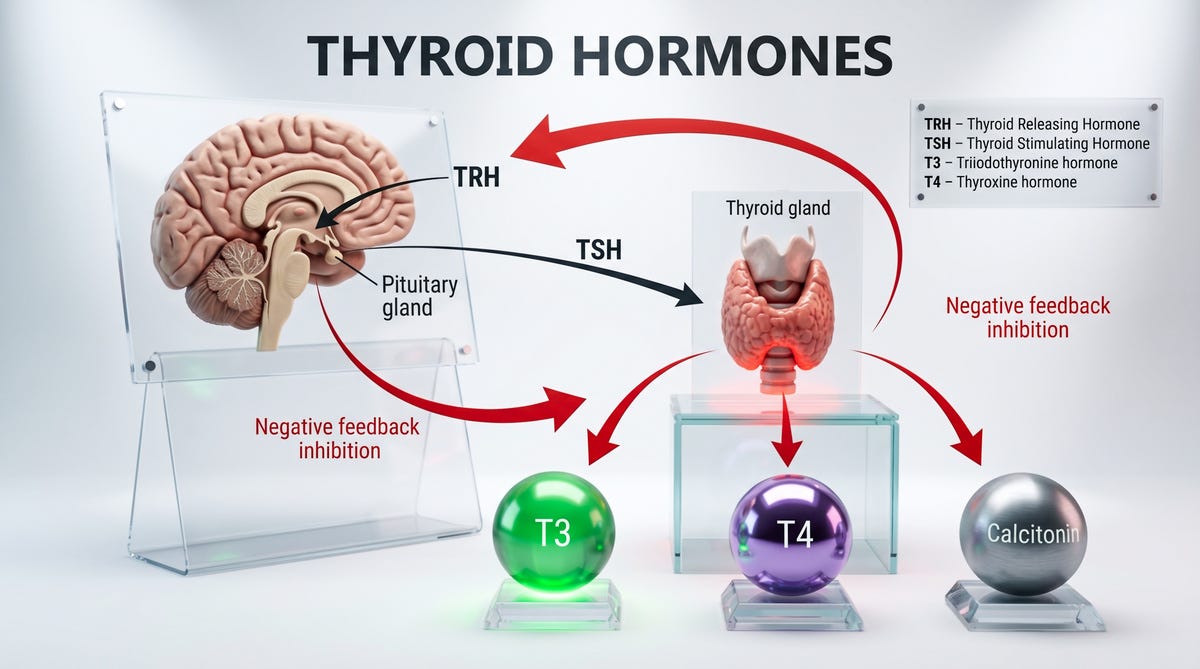
When your GP checks your thyroid, they almost always run a single marker called TSH — thyroid stimulating hormone. TSH is produced by the brain’s pituitary gland, and its job is to tell your thyroid to make more hormone. So the logic goes: if TSH is in the normal range, the thyroid is doing its job.
Here’s where it gets more nuanced.
Your thyroid produces a hormone called T4 (thyroxine). T4 is essentially a storage hormone — it circulates in your blood but isn’t particularly active on its own. For your cells to actually use thyroid hormone, your body needs to convert T4 into T3, its active form. T3 is what regulates your metabolism, your energy, your mood, your body temperature, and your ability to think clearly.
This conversion doesn’t happen in the thyroid. It happens in your tissues — primarily in the liver, gut, and kidneys. And it depends almost entirely on whether your body has the right nutritional building blocks to do the job.
So you can have a perfectly normal TSH reading, a thyroid that’s technically producing enough T4, and still feel every single symptom of an underactive thyroid — because the conversion step is where things are falling apart.
The gap the test doesn’t see
Research has consistently shown that a meaningful proportion of patients with normalised TSH levels still report persistent fatigue, brain fog, low mood, and weight gain. One 2025 review noted that even when TSH is within the target range, around 10–15% of people on thyroid treatment continue to experience symptoms — because normal TSH doesn’t guarantee that T4 is successfully converting to active T3 at the cellular level.
This isn’t fringe thinking. It’s an increasingly recognised issue in clinical endocrinology, with growing interest in whether TSH alone is really sufficient to judge thyroid health — or whether we need to be looking at the full picture, including free T3, free T4, and the ratio between them.
But unless you’re already diagnosed with hypothyroidism and your GP has reason to dig further, these additional markers often aren’t tested. You get the headline number, and if it’s normal, the conversation stops there.
Where things can go wrong (even with a normal TSH)
There are a few distinct scenarios worth understanding:
1. Subclinical hypothyroidism This is where TSH is slightly elevated — the brain is essentially working harder to push the thyroid to produce enough hormone — but T4 is still technically in the normal range. You may or may not have symptoms. Many GPs won’t treat at this stage unless TSH climbs above a certain threshold, meaning people can sit in this grey zone for years, feeling off but getting no support.
2. Poor T4 to T3 conversion Even with a normal TSH and normal T4, the conversion step can be compromised. This can happen due to nutritional deficiencies (more on this below), chronic stress, inflammation, gut dysfunction, or liver strain. Your body may also convert more T4 into something called reverse T3 — a molecule that essentially blocks thyroid receptors and slows everything down — rather than into active T3. Standard blood tests don’t measure this.
3. Hashimoto’s thyroiditis This is an autoimmune condition where the immune system attacks thyroid tissue. It’s the most common cause of hypothyroidism in the UK and can exist — sometimes for years — before TSH shifts enough to trigger a diagnosis. The antibody markers for Hashimoto’s (TPO antibodies and thyroglobulin antibodies) aren’t part of a routine thyroid screen. If you’re symptomatic but your TSH is “normal,” this is worth investigating.
The nutritional piece that most people miss
This is where functional nutrition has a lot to offer, because the conversion of T4 to T3 is a nutrient-dependent process. Without specific micronutrients, those conversion enzymes simply can’t work properly — and no amount of thyroid hormone production will compensate for that.
Selenium is arguably the most important. The enzymes responsible for converting T4 into active T3 — called deiodinases — are selenoproteins. They literally require selenium to function. Research published in 2025 confirms that selenium is essential for both thyroid hormone production and the T4-to-T3 conversion process, and that deficiency is directly linked to impaired conversion. UK soil tends to be relatively low in selenium compared to countries like Brazil or the US, which means dietary intake is often insufficient — and most people have no idea.
Zinc works alongside selenium as a required cofactor for the same conversion enzymes. It also plays a role in thyroid hormone receptor sensitivity — meaning even if you have enough T3, your cells need adequate zinc to actually respond to it. Low zinc is common, particularly in people who don’t eat red meat or shellfish regularly.
Iron (ferritin) is one that often flies under the radar in thyroid conversations. Iron is needed both for the production of thyroid hormone and for the conversion process. Low ferritin — even when haemoglobin is technically normal — is associated with impaired thyroid function. Given how common low ferritin is, especially in women of reproductive age, this connection matters.
Iodine is the mineral most people associate with the thyroid (it makes up the literal backbone of thyroid hormone molecules), but it’s a double-edged sword. Too little impairs hormone production; too much, particularly in people with Hashimoto’s, can actually inflame the thyroid further. In the UK, iodine intake has declined since full-fat dairy consumption dropped, and is a genuine concern — but supplementing blindly without testing is not the answer here.
Vitamin D affects thyroid function through its role in immune regulation. Given that many thyroid conditions are autoimmune in nature, and given that the UK population is chronically low in vitamin D (especially outside summer), this is a relevant and often overlooked piece.
What to actually do with this information
If you’ve been told your thyroid is fine but you recognise yourself in this article, here’s a practical starting point.
Ask for more specific testing. When you next speak to your GP, you can ask whether it’s possible to test free T3 and free T4, not just TSH. You can also ask about TPO antibodies, particularly if there’s any autoimmune condition in your family history. Some GPs will agree; others may refer you. Private testing through companies like Medichecks or Thriva allows you to run a comprehensive thyroid panel without a referral, typically for £50–80.
Look at your nutritional status. Given how central selenium, zinc, iron, and iodine are to thyroid function, it’s worth asking your GP to check ferritin specifically (not just iron or haemoglobin), and vitamin D. Selenium and zinc are harder to test meaningfully via blood (tissue levels are more relevant), but dietary assessment can give a good indication of whether intake is likely adequate.
Support the conversion pathways through food. Brazil nuts are one of the richest dietary sources of selenium — a couple a day provides a meaningful amount. Pumpkin seeds, eggs, legumes, and wholegrains provide zinc. Dairy, eggs, and white fish (particularly haddock and cod) are good UK sources of iodine. Optimising liver function through reduced alcohol, adequate hydration, and bitter greens supports the conversion process too.
Consider the stress and inflammation load. Chronic stress raises cortisol, which directly impairs T4 to T3 conversion. Poor gut health reduces the conversion that happens in the gut (around 20% of T3 is activated there). If you’re working on thyroid health, you can’t separate it from stress, sleep, and gut function — they’re all part of the same picture.
The bottom line
Normal TSH does not automatically mean your thyroid system is working well. It means the signal being sent from your brain to your thyroid is within a certain statistical range. It says nothing about whether T4 is converting efficiently into active T3, whether you have early autoimmune activity, or whether your cells are actually responding to the thyroid hormone in circulation.
If you feel like something is wrong, and your thyroid test keeps coming back fine, you’re not making it up. You’re looking in the right place — you just need someone to look more carefully.
In a paid follow-up to this piece, I go deeper into the functional testing options worth considering, how to interpret a full thyroid panel, and the specific supplementation and dietary protocols that support optimal thyroid conversion — including what to do if you’re on levothyroxine and still don’t feel right.